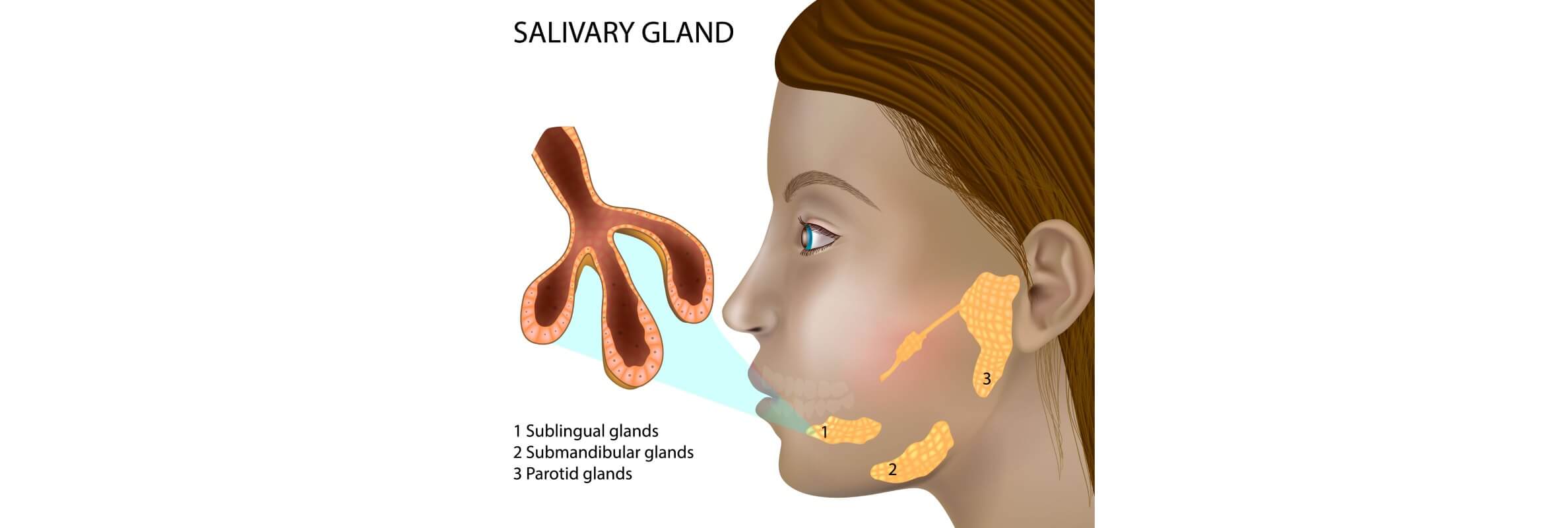

На долю злокачественных новообразований слюнных желез приходится от 0,5 до 1,2% всех случаев рака и 5% случаев опухолей головы и шеи. Опухоли слюнных желез чаще встречаются у женщин: соотношение заболеваемости у мужчин и женщин составляет 1 к 1,5. Примерно 21,7% всех новообразований слюнных желез оказываются злокачественными. Большинство злокачественных поражений при опухолях головы и шеи локализуются в крупных слюнных железах (КСЖ): в первую очередь в околоушных железах, затем по убыванию в подчелюстных железах, подъязычных железах и мелких слюнных железах (МСЖ) [1].
Рак слюнных желез и его особенности
Рак слюнных желез (опухоли слюнных желез) – редкая группа сложных, гетерогенных гистологических новообразований с локализацией в околоушных железах, подчелюстных железах, подъязычных железах и малых слюнных железах верхних отделов дыхательных путей и пищеварительного тракта. К редким типам рака головы и шеи относятся злокачественные опухоли слюнных желез, аденоидно-кистозная карцинома, мукоэпидермоидная карцинома и другие редкие гистологические типы новообразований, при которых пациенту требуется индивидуальный и междисциплинарный подход к лечению.
Разнообразие этиологии, микроскопической гистологии, типов роста и характеристик опухолей слюнных желез нередко затрудняет их диагностику и лечение. Всемирная организация здравоохранения в 2005 году выделила 24 различных злокачественных новообразования слюнных желез: к числу наиболее распространенных гистологических типов относятся мукоэпидермоидная карцинома (MucoCa), ацинарноклеточная карцинома, аденоидно-кистозная карцинома (AКК), эксплеоморфная аденома и аденокарцинома [2]. Плоскоклеточный рак слюнных желез встречается реже, чем мукоэпидермоидная карцинома, но несмотря на тот факт, что это редкое заболевание, оно обычно характеризуется более агрессивным клиническим течением.
Мукоэпидермоидная карцинома (МЭК)
Это наиболее распространенный тип рака слюнных желез (чаще всего поражает крупнейшие слюнные железы). Опухоль образуется из клеток, вырабатывающих слизь, и клеток, сходных с клетками кожи. Внешне она может напоминать костное новообразование или «пузырек с жидкостью». Нередко такие опухоли в течение длительного времени не вызывают серьезных симптомов. Существуют медленно растущие (низкого риска) и более агрессивные формы этого рака желез (слюнных). Более плотное расположение клеток в опухоли обычно связано с более агрессивным поведением заболевания. При развитии такого типа рака в подчелюстных железах во многих случаях требуется проведение более интенсивного курса лечения.
Аденоидно-кистозная карцинома (АКК)
Это медленно растущий, но коварный тип большинства опухолей слюнных желез. Годами размер опухоли может практически не увеличиваться, но при этом новообразование обладает специфической способностью распространяться по нервам. Именно поэтому пациенты иногда испытывают болевые ощущения, покалывание или онемение. Некоторые формы этого рака желез (слюнных) ведут себя более «спокойно», тогда как другие характеризуются гораздо более агрессивным течением и могут метастазировать через кровь. Даже при медленном росте опухоли пациентам с этим типом рака слюнных желез требуется пристальное и длительного врачебное наблюдение.
Ацинарно-клеточная карцинома
Этот вид рака возникает из клеток, которые в норме вырабатывают слюну. Большинство случаев рака слюнных желез этого типа характеризуются медленным ростом и относительно благоприятным прогнозом.
Однако в редких случаях новообразование может изменить свое поведение и трансформироваться в более агрессивное заболевание, в связи с чем даже после успешного лечения важно регулярно проходить контрольные обследования.
Развитие карциномы на фоне плеоморфной аденомы
Этот вид рака развивается из ранее существовавших доброкачественных опухолей слюнных желез, которые присутствовали в организме в течение многих лет. В определенный момент часть клеток «дегенерирует» и начинает проявлять злокачественные свойства. Риск трансформации плеоморфной аденомы в карциному зависит от того, насколько сильно рак распространяется за пределы первичной опухоли: при значительном распространении вероятность развития рецидива и метастазирования выше, а также требуется применение комплексного подхода к лечению.
Что касается доброкачественных опухолей слюнных желез, наиболее распространенной из них является плеоморфная аденома. Новообразование характеризуется медленными темпами роста, преимущественно не вызывает болевых ощущений и часто в течение многих лет выглядит как нормальное уплотнение в области возле уха, под челюстью или на нёбе. Чаще всего встречается у женщин в возрасте 30–50 лет. Хотя опухоль является доброкачественной, важно удалить ее полностью, так как при неполном удалении она может появиться снова или, в очень редких случаях, спустя много лет начать вести себя более агрессивно.
Опухоль Вартина – вторая по распространенности доброкачественная опухоль слюнных желез. К доброкачественным опухолям также относятся миоэпителиома, лимфаденома, аденома сальных желез, онкоцитома, цистаденома и другие типы.
Симптомы и ранние признаки рака слюнных желез
На начальной стадии заболевания симптомы практически отсутствуют. Опухоль слюнной железы может быть подвижной или, наоборот, плотно прилегать к окружающим тканям, ввиду чего не всегда есть возможность сразу отличить злокачественные опухоли слюнных желез от доброкачественных. По этой причине любое новое или подозрительное новообразование в области слюнных желез требует обследования.
По мере прогрессирования заболевания могут появиться болевые ощущения, дискомфорт при жевании или глотании, чувство тяжести в нёбе или глубинных отделах горла, ограничения при раскрытии рта, изменения кожи в области над опухолью, язвы или даже свищи. При локализации опухоли в мелких слюнных железах полости рта она может выглядеть как подслизистое уплотнение, иногда с изъязвлением, тогда как при ее локализации в носовой полости или носоглотке возможны заложенность носа и носовое кровотечение.
Симптомы рака слюнных желез
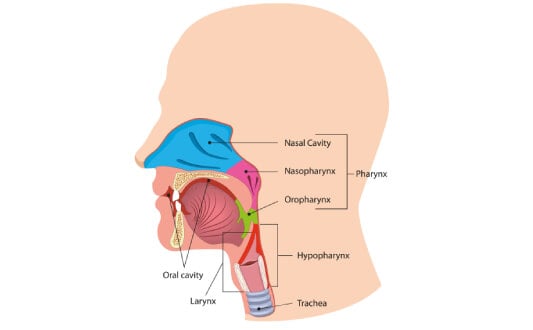
Опухоли мелких слюнных желез глотки или гортани могут проявляться затруднением глотания, болью при глотании, охриплостью голоса, одышкой или ощущением нехватки воздуха. При постепенном усилении подобных симптомов особенно важно не игнорировать их и обратиться к врачу.
К тревожным признакам, которые могут указывать на злокачественный характер новообразования, относятся стремительное увеличение размера опухоли, болевой синдром, снижение подвижности лицевых мышц (слабость или асимметрия), увеличение лимфатических узлов на шее.
При опухолях околоушных желез (раке околоушной железы) появление крупного плотного образования в области перед ухом может сочетаться с повреждением лимфатических узлов шеи. У отдельных пациентов наблюдается паралич лицевого нерва, который проявляется косоглазием, опущением уголков рта или неспособностью закрыть глаз.
Новообразования подчелюстных желез часто проявляются в виде безболезненного уплотнения на шее, которое со временем становится плотным, бугристым и может прорастать в кожу или более глуболежащие ткани. В отдельных случаях также наблюдаются поражения нервов, на фоне которых возникает ряд симптомов: онемение языка, нарушение речи или затруднение глотания.
Опухоли подъязычных желез преимущественно проявляются в виде безболезненного образования на дне полости рта, однако примерно у половины пациентов все же могут наблюдаться болевые ощущения или онемение [3].
Диагностика опухолей слюнных желез
Перед выбором оптимальной тактики лечения необходимо достоверно установить тип опухоли слюнных желез. На первый взгляд такие новообразования могут казаться одинаковыми, но на самом деле они имеют совершенно разные характеристики и специфику клинического течения. Именно поэтому при подозрении на рак слюнных желез всегда требуется проведение поэтапной и комплексной диагностики, сочетающей клиническое обследование, современные визуализационные исследования и морфологический анализ для подтверждения диагноза. Такой подход позволяет не только отличить доброкачественную опухоль от злокачественной, но также определить ее тип, степень распространенности и наиболее эффективный вариант лечения. В отличие от педиатрических форм заболевания, рак слюнных желез у взрослых чаще ассоциируется с агрессивными гистологическими типами и требует междисциплинарного подхода к лечению.
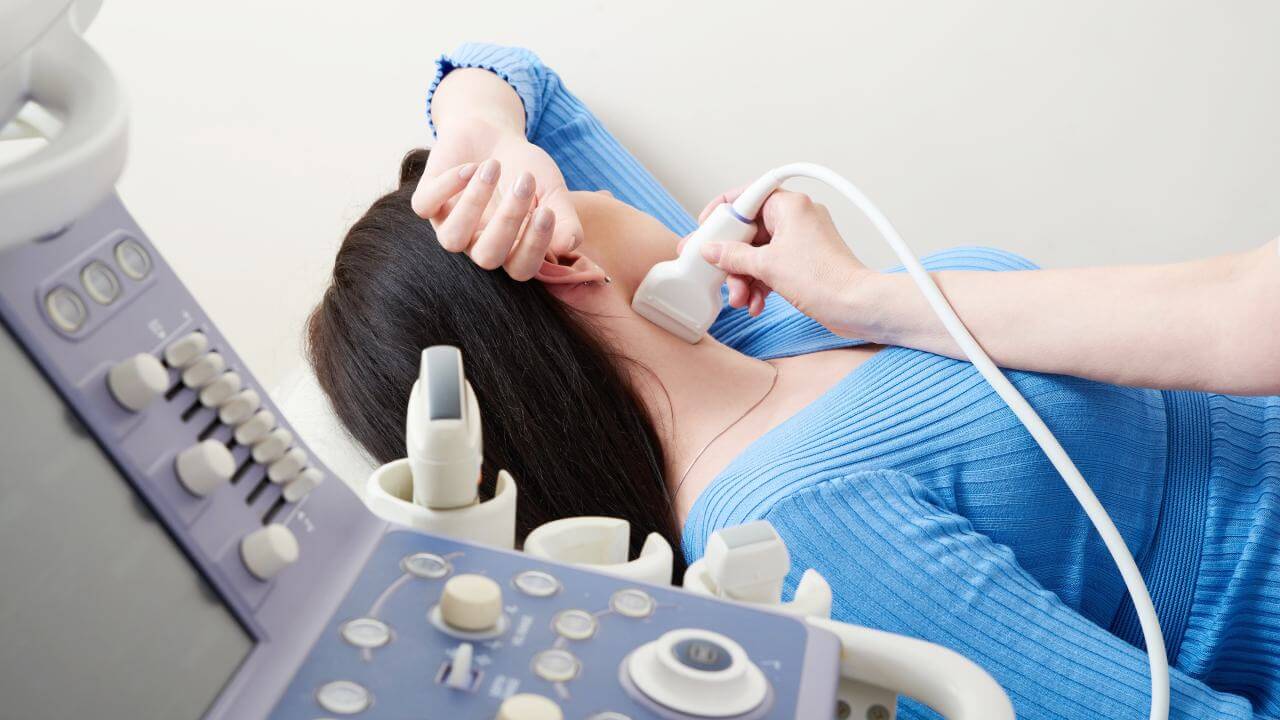
Ультразвуковое исследование – главный неинвазивный метод диагностики для оценки опухолей крупных слюнных желез, особенно поверхностных новообразований околоушных желез. УЗИ помогает определить точную локализацию опухоли и отличить солидные новообразования от кистозных скоплений, а также используется при проведении тонкоигольной аспирационной биопсии. Гетерогенная эхогенность, локальная инвазия, нечеткие границы и лимфаденопатия являются сонографическими признаками, указывающими на злокачественный характер опухоли [4].
Рутинная КТ – позволяет оценить степень распространения опухоли шеи и головы, инфильтрацию костной ткани и лимфаденопатию. Однако возможности КТ ограничены из-за зубных артефактов и недостаточно высокого разрешения для визуализации мягких тканей, особенно при миоэпителиальной карциноме (МЭК), аденоидно-кистозной карциноме (АКК) и ацинарно-клеточной карциноме (АКК), в связи с чем метод не способен обеспечить исчерпывающие данные об опухоли.
МРТ – для оценки степени распространения опухоли, инвазии мягких тканей и повреждения нервов при поражениях глубокой доли околоушных желез, подъязычных желез и мелких слюнных желез рекомендуется проведение магнитно-резонансной томографии (МРТ).
Роль ПЭТ заключается в выявлении локальных и отдаленных метастазов. Благодаря более высоким стандартизированным значениям поглощения тканями, ПЭТ по сравнению с традиционной КТ с более высокой степенью точности визуализирует степень распространения опухоли, поражение лимфоидных узлов, локальные рецидивы и отдаленные метастазы.
Однако ПЭТ не способна дифференцировать доброкачественные и злокачественные опухоли слюнных желез, так как доброкачественные опухоли (например, плеоморфная аденома и опухоль Вартина) демонстрируют высокий уровень поглощения глюкозы из-за наличия в них клеток с высоким содержанием митохондрий [5].
С помощью методов диагностической визуализации нельзя достоверно определить, является ли опухоль доброкачественной или злокачественной, поэтому ключевое значение для выбора дальнейшей тактики лечения имеет получение образцов ткани для проведения гистологического исследования. Инцизионная биопсия выполняется при подозрении на опухоль с локализацией в мелких слюнных железах в ротовой полости, однако эту процедуру не рекомендуется проводить при новообразованиях околоушных желез из-за риска повреждения лицевого нерва и инсеминации опухолевых клеток. Следовательно, предпочтительным вариантом в таком случае является тонкоигольная аспирационная биопсия (ТАБ) под контролем УЗИ.
Стадии рака слюнных желез
Определение стадии заболевания позволяет установить, насколько рак распространяется на момент постановки диагноза. Это принципиально важно, поскольку стадия заболевания влияет на выбор вариантов лечения и прогноз.
Стадия I – локализованный рак
Первая стадия характеризуется образованием опухоли небольшого размера с ее локализацией исключительно в пределах слюнной железы, из которой она возникла. Новообразование не прорастает в соседние ткани, не поражает лимфатические узлы и не распространяется на другие органы. Во многих случаях на этой стадии опухоль выглядит как медленно растущее уплотнение, не вызывающее болевых ощущений или других выраженных симптомов. Как правило, именно на этой стадии обеспечивается максимально эффективное лечение заболевания с наиболее благоприятным прогнозом.
Стадия II – локализованная опухоль крупных размеров
На второй стадии заболевания также констатируется наличие локализованной опухоли, но уже более крупных размеров. Новообразование по-прежнему ограничено слюнной железой и не распространяется на лимфатические узлы или другие органы. У отдельных пациентов на той стадии может возникать чувство давления, дискомфорт или асимметрия лица, но в целом опухоль считается операбельной и хорошо поддается лечению.
Стадия III – местнораспространенный рак
На третьей стадии опухоль либо увеличивается в размерах, либо начинает распространяться на близлежащие лимфатические узлы шеи. Существует риск выхода новообразования за пределы самой железы и поражения соседних тканей. На этой стадии обычно проявляются более выраженные симптомы: болевые ощущения, затруднение глотания, трудности при раскрытии рта, изменения мимики. На третьей стадии констатируется местнораспространенный рак, для лечения которого часто требуется сочетание хирургического вмешательства с лучевой терапией, а в отдельных случаях и другими методами.
Стадия IV – прогрессирующий или метастатический рак
Четвертая стадия характеризуется несколькими вариантами клинического течения заболевания. В некоторых случаях опухоль прорастает глубоко в окружающие структуры – кожу, кости, нервы или другие важные анатомические области. В других клинических ситуациях рак распространяется сразу на несколько крупных лимфатических узлов. При проникновении опухолевых клеток в отдаленные органы, в частности в легкие, кости или печень, диагностируется так называемый метастатический рак.
При метастатическом раке слюнных желез заболевание выходит за пределы области головы и шеи. На этой стадии обычно проводится комплексное лечение, направленное не только на достижение контроля над опухолью, но и на сохранение качества жизни онкобольного.
Стандартные методы лечения рака слюнных желез
Схема стандартного лечения рака слюнных желез всегда подбирается для пациента в индивидуальном порядке. При ее выборе учитывается не один фактор, а комбинация нескольких важных характеристик опухоли: врачи-онкологи принимают во внимание стадию заболевания, тип опухоли и вид слюнных желез, пораженных онкопроцессом, агрессивность новообразования (степень дифференцировки) и его точную локализацию. Специалисты также определяют, можно ли лечить рак слюнных желез с проведением операции по полному удалению опухоли. Кроме того, важное значение придается таким факторам, как общее состояние пациента, функция нервов и возможные последствия лечения для внешнего вида и качества жизни человека.
На первой стадии рак обычно локализован и не распространяется за пределы слюнной железы, поэтому во многих случаях он считается излечимым. Основным лечением низкоагрессивных опухолей является хирургическая операция по удалению новообразования. В большинстве ситуаций этого достаточно для полного выздоровления пациента. При неполном удалении опухоли во время операции или если повторное хирургическое вмешательство потенциально может привести к серьезному нарушению функционального статуса или значительным косметическим дефектам, врачи могут дополнительно рекомендовать проведение лучевой терапии [6]. Дистанционная лучевая терапия, в частности фотонная лучевая терапия, широко применяется в лечении рака слюнных желез в качестве адъювантного или радикального терапевтического метода для улучшения локального контроля над опухолью и снижения риска развития рецидива с максимальным сохранением окружающих здоровых тканей.
При более агрессивных опухолях различных видов слюнных желез даже на первой стадии может потребоваться более расширенный курс лечения. Основу терапевтической схемы в таких случаях по-прежнему составляет хирургическое вмешательство, но после него врачи нередко рекомендуют проведение лучевой терапии, особенно при локализации новообразования вблизи нервных структур или если есть сомнения по поводу его полного удаления во время операции. Такой подход способствует снижению риска развития рецидива заболевания и улучшению контроля над онкопроцессом.
На стадии III рак считается местнораспространенным, поэтому для борьбы с ним обычно проводится комбинированное лечение [7].
Независимо от агрессивности опухоли, основным методом лечения на этой стадии по-прежнему остается хирургическое вмешательство по удалению первичной опухоли, а при необходимости – и пораженных лимфатических узлов шеи. В большинстве случаев после операции рекомендуется проведение лучевой терапии, особенно если опухоль распространилась на лимфатические узлы, наблюдается инвазия новообразования в нервные структуры или констатируется неполное хирургическое удаление опухоли во время вмешательства. При плоскоклеточном раке слюнных желез нередко наблюдается периневральная инвазия и поражение регионарных лимфатических узлов, что влияет на выбор тактики лечения.
При неоперабельных или рецидивирующих опухолях, а также при отсутствии ответа на стандартное лечение, лучевая терапия может применяться как основное лечение или в паллиативных целях. В специализированных центрах проводятся продолжительные курсы лучевой терапии, обеспечивающие более эффективные результаты лечения в сложных клинических ситуациях.
В основе лечения лимфомы слюнных желез лежит химиотерапия, однако этот метод не обладает достаточной эффективностью для борьбы с другими злокачественными опухолями слюнных желез. В ряде исследований при проведении паллиативной химиотерапии у пациентов с противопоказаниями к хирургическому вмешательству или облучению частичный ответ был достигнут лишь в 20-25% случаев [8].
При рецидивирующем раке слюнных желез выбор терапевтической тактики определяется в зависимости от локализации рецидива, гистологического типа опухоли слюнной железы и потенциальной возможности повторного применения локорегионарных методов лечения.
Передовые и инновационные методы лечения рака слюнных желез в Германии
Регионарная химиотерапия
Передовое лечение рака слюнных желез основано на использовании инновационных комбинированных подходов, в частности таргетной терапии, иммунотерапии, регионарной химиотерапии и современных видов лучевой терапии, которые в комплексе позволяют добиться лучшего контроля над заболеванием и сохранить качество жизни пациента. При стандартном подходе химиотерапевтические препараты вводятся внутривенно. Время проведения инфузии может составлять от 30 минут до нескольких часов. Лекарственные препараты системно распределяются с током крови, поэтому их концентрация в опухоли сопоставима с концентрацией в других тканях организма.
В настоящее время пациентам также предлагается инновационное лечение методом регионарной химиотерапии – альтернатива внутриартериальной инфузии химиопрепаратов. В отличие от традиционного внутривенного введения, лекарственные средства доставляются непосредственно к артерии, питающей опухоль. За счет этого обеспечивается достижение высокой концентрации препаратов непосредственно в опухолевом очаге при их значительно меньшем воздействии на весь организм пациента. Данный подход способствует снижению общего числа побочных эффектов при высоких показателях эффективности лечения.
Опыт применения внутриартериальной химиотерапии в условиях реальной клинической практики показывает, что у отдельных пациентов процедура позволяет избежать трахеостомии и исключить необходимость зондового питания, а также способствует стремительному уменьшению размера опухоли и сохранению достойного качества жизни. В то же время для проведения этого метода лечения требуется специализированное оборудование и соответствующий опыт. Важно отметить, что регионарная химиотерапия не является стандартным лечением, которое подходит всем пациентам. Главной отличительной особенностью кратковременной внутриартериальной инфузии является время ее проведения, составляющее всего 5-12 минут.
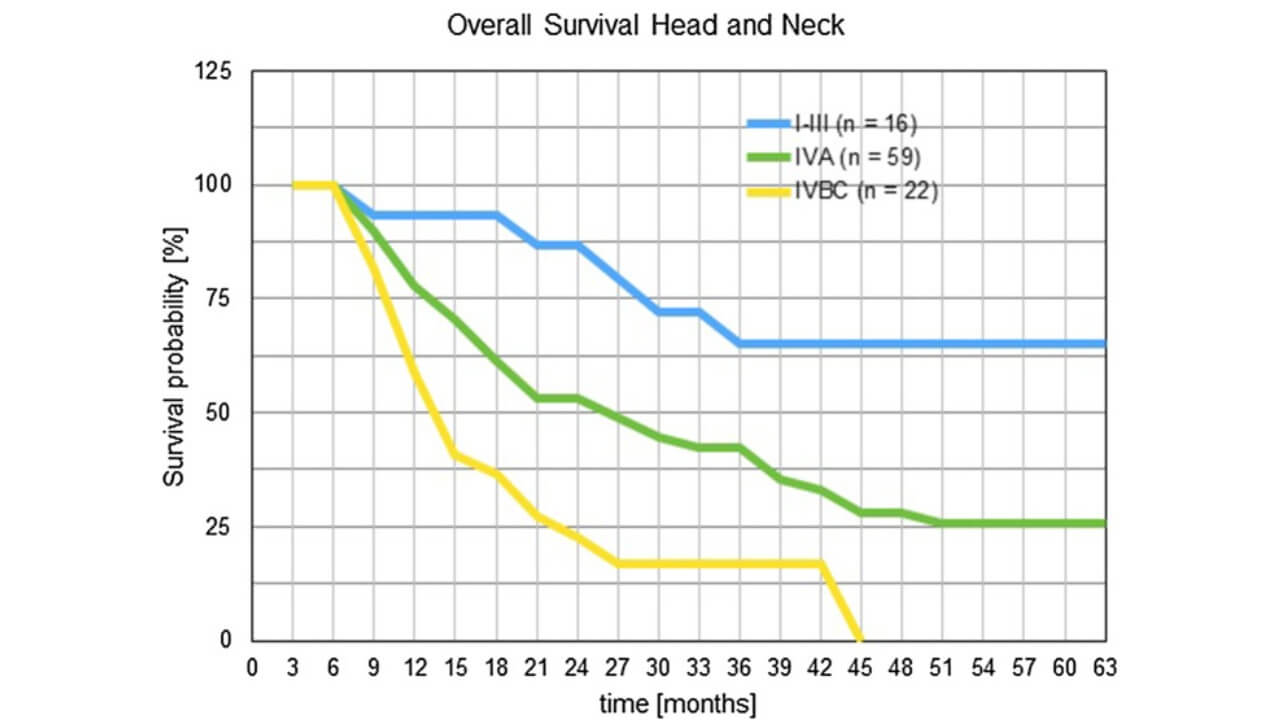
Проведен ряд исследований, в рамках которых пациенты с опухолями головы и шеи проходили процедуры кратковременной внутриартериальной инфузионной химиотерапии. Однолетняя выживаемость пациентов со стадиями опухолей шеи и головы IVB/C, IVA и I–III составила 59%, 82% и 93% соответственно. Двухлетняя выживаемость при этих же стадиях заболевания была на уровне 22%, 53% и 86%. Показатели трехлетней выживаемости снизились до 17%, 42% и 65% соответственно [9].
Терапия дендритными клетками
Терапия дендритными клетками – это один из методов иммунотерапии. Принцип такого лечения основан не на прямом воздействии на опухоль, а на активации защитных механизмов собственной иммунной системы человека, благодаря чему она приобретает способность самостоятельно распознавать и уничтожать раковые клетки.
Дендритные клетки выступают в роли своеобразных «проводников» иммунного ответа: их задача заключается в представлении иммунной системе потенциально опасных «мишеней» (раковых клеток). В 2011 году американскому иммунологу Ральфу Штейнману была присуждена Нобелевская премия за открытие роли дендритных клеток в регуляции иммунного ответа [10], что свидетельствует о важнейшем значении этого открытия для современной медицины и онкологии.
Суть метода состоит в следующем: осуществляется забор собственных иммунных клеток пациента, после чего в лабораторных условиях из них выделяют дендритные клетки, «обучают» их распознавать опухолевые антигены и вводят в организм пациента. При попадании в организм онкобольного дендритные клетки активируют Т-лимфоциты, которые начинают целенаправленно атаковать раковые клетки.
Терапия дендритными клетками рассматривается в качестве вспомогательного или инновационный метода лечения, особенно если речь идет о рецидивирующем или метастатическом раке слюнных желез, когда возможности стандартных методов исчерпаны или не дают ожидаемого эффекта. Кроме того, такой вариант лечения применяется в рамках персонализированных программ иммунотерапии.
При опухолях слюнных желез дендритные клетки, наряду с макрофагами и лимфоцитами, играют важную роль в регуляции иммунного ответа против раковых клеток в микроокружении новообразования. Взаимодействие эпителиальных и мезенхимальных компонентов имеет решающее значение для роста опухоли, при этом дендритные клетки регулируют иммунный ответ в этом процессе [11].
Ученые провели исследование, в ходе которого было продемонстрировано, что участие дендритных клеток на различных стадиях их созревания в большинстве опухолей слюнных желез может служить важным прогностическим маркером и потенциальной мишенью для противоопухолевой терапии.
Электрохимиотерапия
Современный регионарный метод лечения с клинически доказанной эффективностью. К числу главных преимуществ этой терапевтической процедуры относятся высокая точность, локальное воздействие на опухоль и значительно меньший профиль системных побочных эффектов. Электрохимиотерапия основана на сочетании таргетного введения противоопухолевых препаратов, которые сами по себе плохо проникают в раковые клетки, с подачей краткосрочных электрических импульсов непосредственно к опухолевому очагу.
Под воздействием этих импульсов временно «открываются» мембраны раковых клеток, благодаря чему лекарственные препараты проникают в раковые клетки гораздо более эффективно. В результате процедуры происходит разрушение злокачественных опухолевых клеток при минимальном повреждении окружающих здоровых тканей.
Для обеспечения максимально эффективного результата электрохимиотерапии ключевое значение имеет правильный выбор лекарственного препарата и его дозы, точность проведения запланированного лечения, соблюдение оптимального режима подачи электрических импульсов и правильный подбор электродов. Отдельная роль отводится предварительной оценке распределения электрического поля в опухоли и окружающих тканях. Именно от этого во многом зависит успешный исход лечения [12].
Кроме того, после проведения ЭХТ происходит высвобождение молекул, связанных с повреждением раковых клеток, что приводит к увеличению количества опухолевых антигенов. Это, в свою очередь, способствует усилению иммунного ответа против опухоли и повышению эффективности лекарственных препаратов. Лечение рака за границей в основном выбирают пациенты со сложными или редкими формами заболевания, при которых для достижения успешного результата необходим доступ к медицинскому обслуживанию в высокоспециализированных центрах. Лечение рака за границей ценится за высокие стандарты качества, доступ к современным технологиям, применение инновационных терапевтических подходов и четко структурированную междисциплинарную медицинскую помощь.
Важным фактором при выборе метода лечения рака слюнных желез является доступность метода и его стоимость. Хотя традиционные методы лечения обычно более доступны, они могут требовать продолжительной терапии и значительных финансовых вложений. Напротив, инновационное лечение рака слюнных желез часто доступно только в специализированных центрах и может иметь более высокую начальную стоимость, но порой дает возможность сократить продолжительность курса терапии и снизить дополнительные финансовые затраты. В сравнительной таблице ниже представлены данные о доступности методов лечения рака в разных странах, а также предполагаемая стоимость традиционных и передовых методов лечения рака слюнных желез, что поможет пациентам лучше ориентироваться в возможных вариантах лечения.
| Метод лечения | Стоимость в Германии | Стоимость в США | Стоимость в Великобритании | Стоимость в Австралии |
|---|---|---|---|---|
| Хирургическое лечение | €25,000 - €45,000 | €65,000 - €85,000 | €35,000 - €55,000 | €20,000 - €40,000 |
| Химиотерапия | €80,000 - €150,000 за полный курс | €100,000 - €180,000 за полный курс | €90,000 - €165,000 за полный курс | Не проводится |
| Лучевая терапия | €28,000 - €42,000 | €40,000 - €80,000 | €35,000 - €65,000 | €25,000 - €50,000 |
| Терапия ДК | €20,000 - €38,000 | €100,000 - €150,000 | Не проводится | Не проводится |
| Регионарная химиотерапия | €45,000 per session | €37,000 - €150,000 | €30,000 - €118,000 | Не проводится |
| Электрохимиотерапия | €7,500 - €12,000 per session | €40,000 - €100,000 | €25,000 - €45,000 | Не проводится |
История пациента: личный опыт лечения рака слюнных желез
У Марка сложный онкологический анамнез с длительным течением заболевания. У него была диагностирована карцинома околоушной слюнной железы высокой степени злокачественности с признаками местнораспространенного процесса и периневральной инвазии. На первом этапе терапевтического процесса пациенту было проведено радикальное хирургическое вмешательство с последующей адъювантной лучевой терапией. К сожалению, лечение не дало желаемого результата: через некоторое время у Марка выявили локорегионарный рецидив, сопровождающийся болевым синдромом, отеками в области лица и нарушениями жевания, что привело к значительному ухудшению качества жизни пациента.
Попытки провести системную химиотерапию не увенчались успехом по причине низкой переносимости лечения, развития серьезных побочных эффектов и отсутствия значимого клинического ответа на терапию. Учитывая локализацию опухоли, ранее проведенный курс облучения и высокий риск развития осложнений в виде функциональных нарушений при повторных операциях, пациенту был предложен инновационный регионарный метод лечения – внутриартериальная химиотерапия.
Целью лечения было достижение максимально высокой концентрации цитостатиков непосредственно в опухолевом очаге за счет селективного внутриартериального введения препаратов с их минимальным системным воздействием на организм пациента. Лечение проводилось междисциплинарной командой врачей при участии онкохирурга, интервенционного радиолога, клинического онколога и анестезиолога. Процедура выполнялась под ангиографическим контролем, что позволило с высокой степенью точности определить артерии, питающие опухоль.
Семья пациента отметила четкую координацию лечения, постоянный контакт с командой врачей и доходчивое объяснение каждого этапа терапии, что значительно снизило тревожность и психологическую нагрузку в ходе всего процесса. Уже после первых курсов внутриартериальной химиотерапии было зафиксировано выраженное уменьшение объема опухоли, исчезновение болевого синдрома и улучшение жевательной функции.
По результатам контрольного обследования был достигнут частичный, а затем и полный локальный ответ на лечение – это подтверждают данные клинических и визуализационных исследований. Системные побочные эффекты практически отсутствовали, поэтому не было необходимости в длительной госпитализации или снижении дозы химиопрепаратов. Пациент вернулся к привычной повседневной жизни, у него удовлетворительный функциональный статус, исчезла необходимость в постоянном приеме обезболивающих лекарственных средств.
Семья Марка полностью уверена в правильности выбранной тактики лечения и в высоком профессионализме команды специалистов:
«Мы прошли долгий и сложный путь. После лечения стандартными методами мы практически потеряли надежду. Предложение пройти внутриартериальную химиотерапию стало поворотным моментом в жизни Марка. В Германии лечение направлено не только на излечение болезни, но и на восстановление здоровья человека в целом. Сегодня мы видим результат, о котором можно было только мечтать. К счастью, мы снова можем строить планы на будущее».
Поездка на лечение за границу с Booking Health
Самостоятельный поиск наилучшей тактики лечения с учетом вашей индивидуальной клинической ситуации – довольно сложная задача. Испытав на себе многочисленные курсы лечения, проконсультировавшись со множеством специалистов и испробовав различные терапевтические процедуры, вам может быть трудно сориентироваться во всей предоставленной врачами информации. В таком случае пациенты зачастую выбирают первый же предложенный вариант лечения или соглашаются на лечение с применением стандартизированных терапевтических протоколов, которое повлечет за собой множество побочных эффектов, вместо того, чтобы рассмотреть возможность терапии с помощью инновационных процедур.
Если вы хотите сделать осознанный выбор и получить лечение рака в соответствии с индивидуально разработанной для вас схемой с учетом особенностей вашей конкретной клинической ситуации, проконсультируйтесь с медицинскими специалистами Booking Health. Компания Booking Health уже более 12 лет занимает ведущие позиции в сфере организации лечения за рубежом с применением новейших инноваций в медицине, поэтому ее специалисты обладают огромным опытом в составлении персонализированных комплексных программ лечения рака для каждого пациента. Booking Health пользуется репутацией авторитетной компании, которая предоставляет персонализированный подбор схемы лечения рака слюнных желез и клиники с прямым бронированием приема в медицинском центре и полной поддержкой на каждом этапе лечения – от решения организационных вопросов до помощи в процессе лечения. Мы предлагаем:
- Оценку и анализ медицинских заключений пациента
- Составление индивидуальной программы лечения
- Подбор подходящего медицинского учреждения для лечения
- Подготовку медицинской документации и ее направление в выбранную пациентом для лечения клинику
- Консультации с врачами зарубежной клиники для разработки оптимальной медицинской программы на этапе подготовки к поездке на лечение
- Экспертные консультации во время пребывания в больнице
- Последующее консультирование пациента после его возвращения на родину по завершении медицинской программы
- Решение организационных вопросов в рамках подготовки к поездке на лечение за границу
- Координацию и организацию пребывания пациента в другой стране
- Помощь в оформлении визы и бронировании авиабилетов
- Услуги переводчика и персонального координатора, который будет с вами на связи 24/7
- Прозрачные цены на лечение без скрытых платежей
Здоровье – главная ценность в жизни каждого человека, доверять заботу о которой стоит лишь лучшим специалистам с богатым опытом и проверенной репутацией. Booking Health – это ваш надежный партнер, который оказывает всестороннюю помощь на пути к восстановлению здоровья и улучшению качества жизни. Свяжитесь с медицинским консультантом компании, чтобы узнать больше о возможностях персонализированного лечения рака слюнных желез у ведущих экспертов с использованием инновационных методов.
Успешная борьба с раком: опыт пациентов Booking Health










Частые вопросы о раке слюнных желез
Отправить запрос на лечениеОсновные симптомы рака желез (слюнных) включают безболезненные или болезненные отеки в области лица, шеи или рта, асимметрию лица, затруднение жевания или глотания, онемение, болевые ощущения, слабость лицевого нерва и увеличение лимфатических узлов. Нередко при опухоли слюнной железы на ранних стадиях выраженные симптомы отсутствуют.
Показатели выживаемости при раке слюнных желез определяются такими факторами, как стадия опухоли, ее гистологический тип и степень злокачественности. На ранних стадиях прогноз благоприятный, тогда как при прогрессирующем раке желез (слюнных) отмечаются более низкие показатели выживаемости. Однако даже на поздних стадиях заболевания показатели выживаемости значительно варьируются в зависимости от выбранной тактики лечения.
Да, рак слюнных желез считается излечимым заболеванием, особенно при его выявлении на ранних стадиях и правильном выборе оптимальной схемы лечения, которая обычно предполагает сочетание лучевой терапии с операцией или проведение только одного хирургического вмешательства.
На 1 стадии диагностируется локализованная опухоль слюнной железы, ограниченная пределами слюнной железы, без поражения лимфатических узлов или отдаленных метастазов.
Темпы прогрессирования рака слюнных желез могут различаться: некоторые виды опухолей растут медленно, тогда как другие характеризуются агрессивным ростом, поэтому рак распространяется еще на ранних стадиях. Темпы роста новообразования и распространения раковых клеток слюнных желез зависят от его гистологического типа и стадии заболевания.
Да, рак слюнных желез поддается лечению, при этом лечение слюнных желез возможно даже на поздних стадиях. Современные терапевтические возможности позволяют добиться контроля над заболеванием и поддерживать достойное качество жизни пациентов.
Наиболее эффективным вариантом лечения рака околоушной железы является хирургическое удаление первичной опухоли. При высоком риске развития рецидива операция проводится в комплексе с лучевой терапией. В некоторых случаях в схему лечения пациентов также включают системные или регионарные виды терапии.
Диагноз ставится на основании результатов клинического осмотра, УЗИ, МРТ или КТ, тонкоигольной биопсии или трепан-биопсии и гистологического исследования, проводимого с целью подтверждения наличия у пациента опухоли слюнной железы.
Основные методы лечения рака желез (слюнных) включают хирургическое вмешательство, лучевую терапию, химиотерапию, таргетную терапию и инновационные регионарные процедуры. Оптимальный метод или комплекс методов лечения назначается пациенту в зависимости от стадии и типа рака слюнных желез.
Прогноз при прогрессирующем раке слюнных желез (метастатической опухоли) не такой благоприятный, как на ранних стадиях заболевания, однако при использовании современных комбинированных терапевтических схем и инновационных процедур лечения слюнных желез есть возможность добиться длительного контроля над онкопроцессом.
Да, пациенты с раком шеи и головы, в том числе раком слюнных желез, нередко отдают предпочтение лечению рака за границей, особенно если речь идет о сложных или рецидивирующих опухолях головы и шеи, когда для успешного результата требуется доступ к инновационным методам лечения.
Стоимость лечения рака слюнных желез в Германии определяется в зависимости от таких факторов: стадии заболевания, выбранного метода лечения и продолжительности курса терапии. Общая стоимость лечения может варьироваться от нескольких тысяч до десятков тысяч евро, особенно при применении комбинированных или высокотехнологичных подходов.
Выбирайте лечение за рубежом и Вы, несомненно, получите отличный результат!
Авторы:
Статья составлена под редакцией экспертов в области медицины, врачей-специалистов доктора Надежды Иванисовой и доктора Дарьи Сухорученко. Для лечения состояний, о которых идет речь в статье, необходимо обратиться к врачу; информация в статье не предназначена для самолечения!
С редакционной политикой, которая отражает наше стремление к точности и прозрачности, можно ознакомиться здесь. Перейдите по ссылке, чтобы ознакомиться с нашими правилами.
Источники:
[1] J G Batsakis, J A Regezi. The pathology of head and neck tumors: salivary glands, part 1. Head Neck Surg. 1978 Sep-Oct;1(1):59-68. doi: 10.1002/hed.2890010109. [DOI] [PubMed]
[2] R H Spiro. Salivary neoplasms: overview of a 35-year experience with 2,807 patients. Head Neck Surg. 1986 Jan-Feb;8(3):177-84. doi: 10.1002/hed.2890080309. [DOI] [PubMed]
[3] Patrick J Bradley. Frequency and Histopathology by Site, Major Pathologies, Symptoms and Signs of Salivary Gland Neoplasms. Adv Otorhinolaryngol. 2016:78:9-16. doi: 10.1159/000442120. Epub 2016 Apr 12. [DOI] [PubMed]
[4] M Michal, A Skálová, P Mukensnabl. Micropapillary carcinoma of the parotid gland arising in mucinous cystadenoma. Virchows Arch. 2000 Oct;437(4):465-8. doi: 10.1007/s004280000274. [DOI] [PubMed]
[5] Young Chang Lim, Sei Young Lee, Kyubo Kim et al. Conservative parotidectomy for the treatment of parotid cancers. Oral Oncol. 2005 Nov;41(10):1021-7. doi: 10.1016/j.oraloncology.2005.06.004. Epub 2005 Aug 29. [DOI] [PubMed]
[6] R M Byers, R H Jesse, O M Guillamondegui, M A Luna. Malignant tumors of the submaxillary gland. Am J Surg. 1973 Oct;126(4):458-63. doi: 10.1016/s0002-9610(73)80030-3. [DOI] [PubMed]
[7] C Theriault, P J Fitzpatrick. Malignant parotid tumors. Prognostic factors and optimum treatment. Am J Clin Oncol. 1986 Dec;9(6):510-6. doi: 10.1097/00000421-198612000-00009. [DOI] [PubMed]
[8] C C Wang, M Goodman. Photon irradiation of unresectable carcinomas of salivary glands. Int J Radiat Oncol Biol Phys. 1991 Aug;21(3):569-76. doi: 10.1016/0360-3016(91)90672-q. [DOI] [PubMed]
[9] Karl R Aigner, Emir Selak, Kornelia Aigner. Short-term intra-arterial infusion chemotherapy for head and neck cancer patients maintaining quality of life. J Cancer Res Clin Oncol. 2018 Oct 31;145(1):261–268. doi: 10.1007/s00432-018-2784-4. [DOI] [PMC free articled]
[10] Roman Volchenkov, Florian Sprater, Petra Vogelsang, Silke Appel. The 2011 Nobel Prize in physiology or medicine. Scand J Immunol. 2012 Jan;75(1):1-4. doi: 10.1111/j.1365-3083.2011.02663.x. [DOI] [PubMed]
[11] Wenyue Chen, Zhengqiang Li, Jin Tang, Shuguang Liu. Dendritic cell-based immunotherapy for head and neck squamous cell carcinoma: advances and challenges. Front Immunol. 2025 May 26;16:1573635. doi: 10.3389/fimmu.2025.1573635. [DOI] [PMC free articled]
[12] Arnoldas Morozas, Veronika Malyško-Ptašinskė, Julita Kulbacka et al. Electrochemotherapy for head and neck cancers: possibilities and limitations. Front Oncol. 2024 Feb 15;14:1353800. doi: 10.3389/fonc.2024.1353800. [DOI] [PMC free articled]
[13] Karl R Aigner, Emir Selak, Kornelia Aigne. Short-term intra-arterial infusion chemotherapy for head and neck cancer patients maintaining quality of life. J Cancer Res Clin Oncol. 2019 Jan;145(1):261-268. doi: 10.1007/s00432-018-2784-4. Epub 2018 Oct 31. [DOI] [PubMed]
Читайте: